Atmiyata is a community-led, evidence-based intervention to reduce the mental health and social care gap in communities.
With its innovative and sustainable approach, Atmiyata offers a low-cost, scalable model to improve access to community mental health care.
The World Health Organization has listed Atmiyata as one of the 25 good practices for community outreach mental health services in the world. To know more, click here.
Atmiyata is featured as a case report in the World Health Organization’s report on community-based mental health services in the South-East Asia Region. To know more, click here.

A short film on Atmiyata produced by Mariwala Health Initiative
Why Community-Based Mental Health Matters
In India, close to 14.3% of our population, i.e., 197 million people live with some form of a mental health condition.
The National Mental Health Survey (2016) shows that there exists a large mental health care gap wherein 76-85% of people with mental health conditions in need of mental health care and treatment cannot access the necessary care. This is primarily due to both, demand and supply-related factors.
Demand-related factors: These include stigma, discrimination as well as other structural and social barriers that make it difficult for people to access mental health care.
Supply-related factors: These include the lack of specialised professionals, poor quality of available services, high costs, services that are inaccessible as they are located far away, and a purely bio-medical approach that does not consider socio-cultural factors that influence an individual’s mental health.
This mental health care gap is particularly large in rural areas as many individuals are trapped in a cycle of poverty, social isolation, ill-health, disability, and social exclusion.
How the Atmiyata Model Works
The Atmiyata intervention employs a stepped care approach, using community-based volunteers knowns as Champions, who are identified, trained, and mentored to:
- Provide psychosocial support: Champions provide 4-6 counselling sessions using evidence-based techniques to those with common mental health conditions such as depression and anxiety.
- Make referrals: Refer persons with severe mental health conditions to public mental health services when required.
- Facilitate access to social benefits: Enable access to social care benefits such as pension, disability support, etc. to increase financial stability.
- Build awareness: Raise community awareness by using the Atmiyata App to show films based on social determinants of mental health to a small group of 3-4 community members.
Built on the tenets of empathy and volunteerism, Atmiyata equips communities to meet their own mental health and social care needs.
What is the impact?
Atmiyata aims to assist people with common mental health conditions lead productive and healthy lives, breaking the vicious cycle of poverty and mental ill-health. It strives to create a shift in the mental health systems in low-middle-income contexts through its community-led approach.
As a mental health intervention, Atmiyata seeks to reduce the treatment and psychosocial care gap for both common and severe mental health conditions, improve access to benefits and quality of life, and reduce levels of disability.
The effectiveness of the Atmiyata intervention has been evaluated through a Stepped Wedge Cluster Randomised Controlled Trial (SW-CRCT) with a nested economic evaluation from 2017–19. The SW-CRCT results showed that:
- Persons with common mental health conditions receiving the Atmiyata intervention are 3 times more likely to show reduction in symptoms of depression and anxiety, with a sustained effect.
- The Atmiyata intervention is effective in reducing symptoms of depression and anxiety, improving quality of life and social participation.
- Champions (trained community-volunteers) are skilled to identify persons with common mental health conditions with an accuracy of 58%, which improves over time.
The detailed results of the evaluation can be found here.
Our preliminary results show that Atmiyata is also an economically viable model with a return of $9.35 on every $1 invested, we will soon publish the results of the economic evaluation.
Where have we have reached?
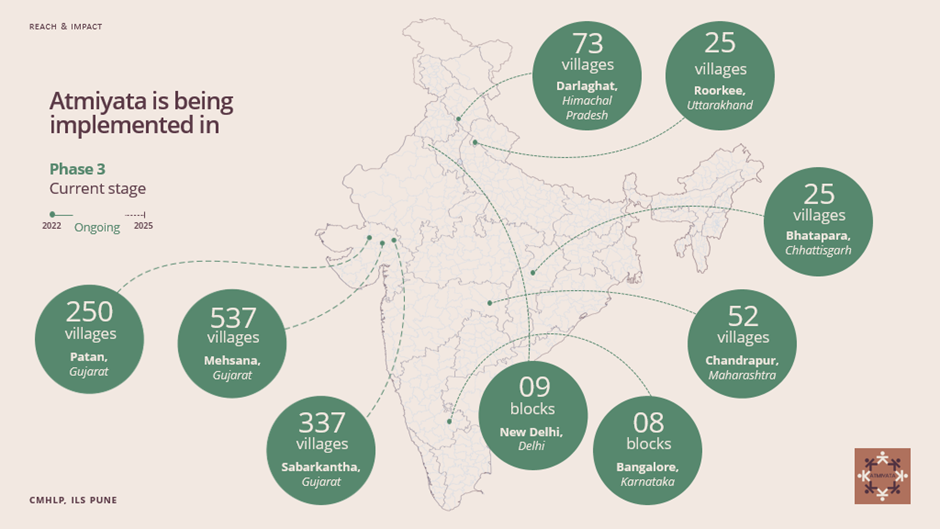
From 2013 to 2015, Atmiyata was piloted as a proof-of-concept study in 41 villages of Nashik district, Maharashtra. Atmiyata was transitioned to scale in Mehsana, district Gujarat across 530 villages.
Direct Implementation and Impact in Rural Communities
Since 2019, Atmiyata is being implemented at scale in Patan and Sabarkantha districts of Gujarat across 1219 villages, reaching approximately 25,000 people with mental health conditions every year. Additionally, we have scaled up Atmiyata through strategic partnerships, where we provide technical support while the partner organization leads the implementation of the intervention.
Partnerships
We have also partnered with Ambuja Foundation, Hasiru Dala, Delhi Commission for Women, and Association for Health Welfare in Nilgiris (ASHWINI) to expand Atmiyata’s reach across diverse geographic and rural settings. We have also entered future partnerships with Kadam Jan Vikas Sanstha, Ambuja Foundation, and the Queen Mary University of London (funded by Barts Charity) to further expand the intervention.
Project Team
Jasmine Kalha, Co-lead,
Kaustubh Joag, Co-lead
Nitish Narkhedkar, Programme Manager
Neeraja Auti, Project Manager
Palak Korde, Project Manager
Funders & Partners
Funded by
Grand Challenges Canada
Mariwala Health Initiative
Collaborator
Health & Family Welfare Department, Govt of Gujarat
Ambuja Foundation
FUNDERS

PARTNERS
