Conditional Cash Transfer programs have not only achieved their objective of poverty and inequality reduction but have also had a desirable effect by significantly reducing suicides.
[This blog post was first published as an article in The New Indian Express]

As machines take over the world, the need for Universal Basic Income (UBI) is a ubiquitous opinion backed by eminent economists like Nobel laureates Peter Diamond and Christopher Pissarides, among others. Even usually bickering Mark Zuckerberg and Elon Musk both agree on the matter of Universal Basic Income.
Although India is still far away from UBI, some low- and middle-income countries, (LMICs) like Brazil, Indonesia, and Kenya have experimented with a modified version of UBI, 'conditional cash transfer (CCT) programs'. CCT programs are considered an effective anti-poverty measure as they are designed to give money to a carefully identified group of people living in extreme poverty. The cash transfer is conditional as it occurs in return for fulfillment of specific behavioural conditions by the beneficiary, such as a commitment to school enrollment.
In most instances we studied, CCT programs have not only achieved their objective of poverty and inequality reduction but have also had a desirable effect by significantly improving mental well-being and reducing suicides among beneficiaries, a remarkable finding.
Evidence from Brazil and Indonesia
Let's look at evidence from Brazil and Indonesia -- countries similar to India in demographic profile. Brazil’s Bolsa Família Program (BFP) is the world's largest CCT program in terms of number of beneficiaries. By the project's closing in December 2018 (version 1), BFP had reached a total of 46.9 million people or about 25% of Brazil’s population. BFP was introduced by the then-president, Lula da Silva, as a government program with the aim to reduce poverty, hunger and inequality. Under the program, low-income families received monthly cash transfers based on their household income and family compositions concurrent to the fulfillment of conditionalities like school attendance for teenagers, immunisation of children, prenatal monitoring of pregnant women and remedial education for children and for those susceptible to be drawn into child labour.
At its inception in 2003, the beneficiary households could receive a monthly benefit of between R$15 (Brazilian Real) and R$95 (US$7-45), depending on the family composition and poverty status. These amounts were changed using PPP (purchasing power parity) conversion factors over the duration of the program. This program resulted in a 58% decline in extreme poverty, a 30% decline in poverty, and a 41% per cent fall in inequality between 2004 and 2014.
Various external studies have validated the positive impact of BFP on human capital outcomes like health, nutrition and survival of targeted individuals. The most exemplary out of these, is a longitudinal study that states -- "data from the 100 million Brazilian Cohort, covering a 12-year period from 2004 to 2015, showed that BFP beneficiaries had a 61% lower suicide rate than non-beneficiaries. This effect was higher among women."
Similar results were obtained from Indonesia. The Program Keluarga Harapan (PHK) or Family Hope Program is Indonesia’s national CCT program, in operation since 2007. It provides a quarterly cash benefit to the poorest 10% of the Indonesian population with children and/or pregnant women. The cash benefit is conditional on children’s school enrollment and attendance, regular health check-ups for kids and pre-natal care for pregnant women.
PKH now also includes a social pension for the elderly aged 70 plus and grants for people with severe disabilities based on certain conditionalities. The households receive grants for 6 years as long as they comply with the conditions and are eligible under the poverty line cut-off. The grant amount was originally variable according to household composition (e.g., the age and number of children) and ranged from a minimum of IDR (Indonesian Rupiah) 800,000 (approximately $61) to a maximum of IDR 3.7 million (approximately $284) per household per year.
Consistent with findings from other CCT programs worldwide, several evaluations conclude that the PKH has been effective in reducing poverty and in improving human capital. And once again, the program’s introduction decreased suicide probability among the beneficiaries by 0.36 per 100,000 individuals equivalent to 18% reduction in suicides.
There is consensus amongst researchers across the world that poverty and mental health are closely associated and CCTs seem to be the perfect pill in the hands of policymakers to reduce suicides.
Suicides in India
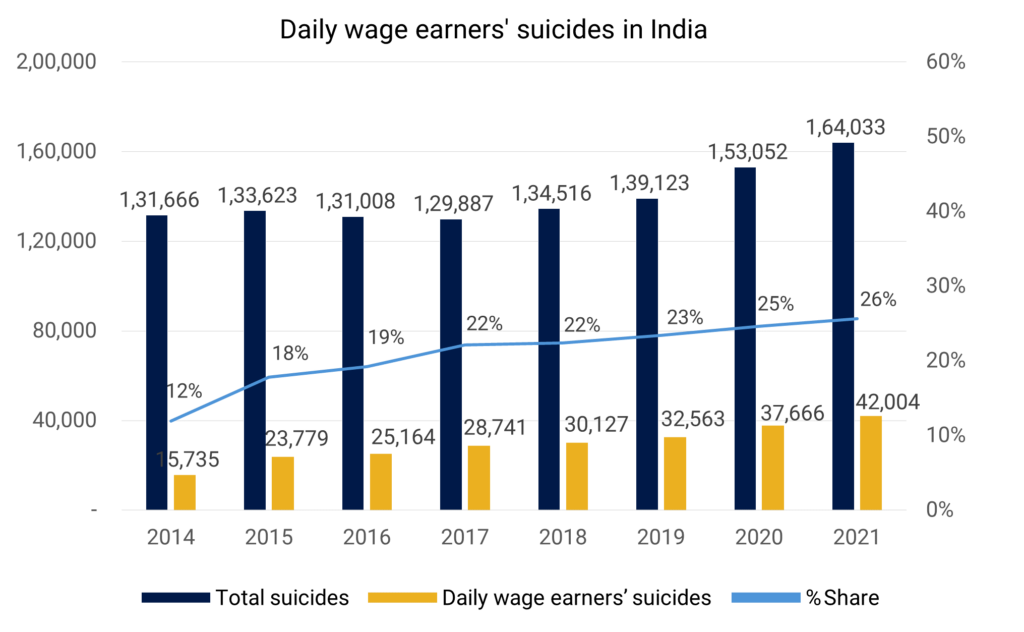
According to the data from the National Crimes Record Bureau (NCRB), there has been a consistent rise in suicides by daily wage earners. What is alarming is, their share in suicides has risen consistently- from 12% of total suicides in India in 2014 to 26% in 2021. In fact, the daily wage earners remained the largest group among suicide victims for two consecutive pandemic years, pointing towards a strong association between economic difficulties and suicides in India.
Ongoing CCT programmes in India
Within India, there have been two CCT programs targeted toward maternal care: a) The Pradhan Mantri Matru Vandana Yojana, and b) the Janani Suraksha Yojana (JSY). Studies conducted show that both programs have started making some difference to mother and infant health in terms of an increase in institutional deliveries, increased immunization and the increased gap between two children.
In one study in Uttar Pradesh, JSY was found beneficial in reducing post-partum depression in women.
However, specific studies targeting suicides and mental health have not yet been conducted in India, despite the country having a huge burden of mental health issues as well as suicides. A small cash transfer trial was conducted in Chennai, Tamil Nadu, India during the peak of the COVID pandemic in 2020-2021 in partnership with SCARF, India (Schizophrenia Research Foundation), the results of which are awaited.
Way forward
Broadly, evidence from across the world shows CCT programs play an important role in poverty reduction and the well-being (and mental health) of targeted populations. Even more remarkable is the significant reduction in suicide rates of targeted populations in examples where this parameter has been measured. The effects of CCT on reducing suicides are large and long-lasting, particularly beneficial for poor individuals and, potentially, women. Additionally, various reviews also indicate that the cost-benefits of cash transfers are favourable even without considering the intangible benefits like positive impact on mental health.
Suicide prevention is a complex issue and CCT can be one possible intervention for a particular stratum of society. Given the unequivocal evidence from other countries, it is time India critically examines and gathers evidence to test CCT as a tool to reduce the extremely high numbers of suicides among the Indian poor.
Sayali Mahashur is a Research Associate and Soumitra Pathare is the Director at the Centre for Mental Health Law & Policy, Indian Law Society, Pune.